Musa DI, Goon DT, Omachi S, Jonathan SU. Aerobic fitness, lipid ratio, visceral adiposity index and risk of hypertension in adolescents: An observational study. World J Clin Pediatr 2025; 14(3): 105939 [DOI: 10.5409/wjcp.v14.i3.105939]
Corresponding Author of This Article
Danladi Ibrahim Musa, PhD, Professor, Department of Human Kinetics and Health Education, Ankpa Road, Kogi State University, Anyigba 272102, Kogi, Nigeria. musa.d@ksu.edu.ng
Research Domain of This Article
Pediatrics
Article-Type of This Article
Observational Study
Open-Access Policy of This Article
This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Author contributions: Musa DI conceived the study, analyzed the data and wrote the draft of the manuscript; Goon DT participated in data analysis, literature search and preparation of the manuscript; Omachi S participated in data collection, literature search, and proofread the manuscript; Jonathan SU participated in literature search and revised the manuscript critically for intellectual content, all authors have read and approved the final draft of the manuscript.
Institutional review board statement: The study was approved by the Ethical Review Committee of the College of Health Sciences, Kogi State University, Nigeria (Ref No: COHS/02/25/2020).
Informed consent statement: Written informed consent from parents/guardians and participants’ assent were obtained before data collection. All tests complied with the ethical guidelines outlined in the Helsinki Declaration as amended.
Conflict-of-interest statement: The authors have no conflict of interest.
STROBE statement: The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement- checklist of items.
Data sharing statement: Technical appendix, statistical code, and dataset available from the corresponding author at dimusa55@gmail.com
Open Access: This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Corresponding author: Danladi Ibrahim Musa, PhD, Professor, Department of Human Kinetics and Health Education, Ankpa Road, Kogi State University, Anyigba 272102, Kogi, Nigeria. musa.d@ksu.edu.ng
Received: February 11, 2025 Revised: March 25, 2025 Accepted: April 15, 2025 Published online: September 9, 2025 Processing time: 125 Days and 22.1 Hours
Abstract
BACKGROUND
Hypertension (HTN) is a significant global health concern due to its rising prevalence and associated risks of cardiovascular disease, chronic kidney disease, and other comorbidities. The increasing rates of HTN among youth have been partly attributed to the global rise in childhood obesity, lipid abnormalities, and sedentary lifestyles.
AIM
To investigate the independent associations of aerobic fitness (AF), the triglyceride-to-high-density lipoprotein cholesterol (TG/HDL-C) ratio, visceral adiposity index (VAI), and resting blood pressure (BP) in Nigerian adolescents.
METHODS
A multistage sampling technique was used to select 403 in-school adolescents aged 11-19 years in Kogi East, Nigeria. Participants were assessed for AF, TG/HDL-C ratio, VAI, systolic BP (SBP), and diastolic BP (DBP). The associations between the independent variables and the risk of systolic and diastolic HTN were examined using multivariate regression models, controlling for age and maturity status. Receiver operating characteristics curve (ROC) and area under the curve (AUC) were employed to determine the predictive capacities of the independent variables.
RESULTS
The overall prevalence of systolic HTN was 5.5% (girls: 7%; boys: 4%) while diastolic HTN was 12.7% (girls: 16.9%; boys: 8.4%). Among girls, all independent variables showed significant associations with SBP, including fitness (P < 0.001), TG/HDL-C (P < 0.001), and VAI (P < 0.001), with VAI showing the strongest association. In boys, all independent variables except VAI (P = 0.063) were significantly associated with SBP, with fitness showing the stronger predictive power (Fitness, P < 0.001; TG/HDL-C, P = 0.029). For DBP, all independent variables, except fitness in girls (P = 0.099), were significantly associated (P < 0.001) in both sexes. Unfit boys were 1.1 times more likely to develop systolic HTN (95%CI: 1.01–1.15, P = 0.018) and had 1.1 times higher odds of developing diastolic HTN (95%CI: 1.03–1.13, P = 0.001). Only the ROC for DBP turned up significant (P < 0.001) AUCs for TG/HDL-C and VAI in girls only, with 0.6 and 1.0 thresholds respectively.
CONCLUSION
AF, dyslipidemia, and visceral adipose tissue dysfunction were independently associated with the risk of HTN in Nigerian adolescents. These findings highlight the importance of promoting a healthy diet and encouraging aerobic physical activity among adolescents to reduce the risk of HTN.
Core Tip: This study examined the independent associations of aerobic fitness (AF), the atherogenic index of plasma (AIP), and the visceral adiposity index (VAI) with resting blood pressure (BP), a key indicator of cardiovascular health. Adolescents with lower AF and elevated AIP and VAI were at an increased risk of HTN. Low fitness, dyslipidemia, and excessive visceral adipose tissue were independently associated with HTN risk. Notably, VAI exhibited a stronger association in girls, while fitness had greater impact in boys. Health promotion efforts should prioritize a balanced diet and regular endurance-based physical activity to support optimal BP levels in adolescents.
Citation: Musa DI, Goon DT, Omachi S, Jonathan SU. Aerobic fitness, lipid ratio, visceral adiposity index and risk of hypertension in adolescents: An observational study. World J Clin Pediatr 2025; 14(3): 105939
Hypertension (HTN), a medical condition characterized by consistently elevated blood pressure (BP) against the arterial walls, is one of the most prevalent risk factors for cardiovascular disease (CVD)[1]. Globally, HTN causes the highest number of deaths, inflicting severe damage to the heart, brain, and kidneys while imposing significant financial burdens on patients and their families[2,3]. HTN is the third most prevalent cause of mortality worldwide and the most predominant risk factor for noncommunicable diseases, accounting for estimated 9.4 million of the 17.7 million annual deaths linked to CVD[4,5]. Epidemiological data indicate approximately one billion HTN patients worldwide, with projections estimating an increase to 1.292 billion by 2025[6]. Alarmingly, HTN is increasingly becoming a concern in pediatric populations, as elevated BP in children is associated with a higher risk of developing target organ damage and CVD in adulthood[2,7]. Once considered rare in Africa, the prevalence of HTN in the region is rising steadily, driven by sedentary lifestyles, weight disorders, and unhealthy diets[8,9].
Although HTN is less frequently observed in children and adolescents, its increasing occurrence in this demographic is alarming, given its potential to persist into adulthood[5]. While the specific etiology of HTN remains nebulous, low physical activity or fitness levels and high body fat are among the major predisposing factors[10,11]. Early detection and management of HTN during childhood are therefore essential for promoting better cardiovascular health outcomes in later life.
Due to the difficulties associated with treating HTN and the health complications it imposes, preventive strategies focusing on lifestyle modifications are prioritized, particularly among younger populations. Common preventive and management strategies include engagement in physical activity, weight control, and dietary interventions[8,12]. Aerobic fitness (AF), an index of habitual physical activity, has been identified as an important determinant of HTN risk. Findings from both cross-sectional[13,14] and longitudinal research[15] highlight an inverse association between AF and elevated BP levels in children and adolescents. In a large-scale study of 3243 children and adolescents in North-Central Nigeria, Musa and Williams[13] reported a negative correlation between low fitness levels and increased systolic BP (SBP) and diastolic BP (DBP).
Although, the rising prevalence of HTN in youth has been attributed to the increasing prevalence of overweight and obesity in this population[16], research indicates that the association between HTN and body weight is related more to fat distribution than excess fat alone[17,18]. While body mass index (BMI) and waist circumference (WC) are frequently used to assess obesity in CVD risk evaluations, these measures have limitations. BMI cannot assess body fat percentage, and WC cannot differentiate visceral adipose tissue (VAT) from subcutaneous adipose tissue (SAT)[19]. Recently, the visceral adiposity index (VAI) has emerged as a surrogate indicator of VAT function and has been shown to correlate with VAT independently of SAT[19]. VAI is now recognized as a predictor of CVD risk factors, including HTN[20,21]. Among the multiple risk factors contributing to CVD, dyslipidemia - an abnormal plasma lipid profile is a major concern[22]. The triglyceride-to-high-density lipoprotein cholesterol (TG/HDL-C) ratio, also known as the atherogenic index of plasma (AIP), is a robust biomarker of metabolic syndrome and coronary atherosclerosis[23]. The combination of hypertriglyceridemia and hypoalphalipoproteinemia, as reflected by AIP, increases the risk of HTN and carotid intima-media thickening[24-26]. In a study of 2721 Korean adolescents, Chu et al[26] documented a strong correlation between the TG/HDL-C ratio and BP levels.
Nigeria, like many countries, is undergoing significant lifestyle transitions, leading to a rise in chronic health problems, even among pediatric populations. While studies on the importance of maintaining healthy lifestyles are common in developed countries, there is a paucity of such research in developing nations, particularly in Africa. As a developing country with limited health facilities to manage HTN, Nigeria faces potentially catastrophic consequences of the disease. This situation underscores the urgent need for studies that examine the associations between key health markers and HTN risk in youth populations to mitigate the future burden of the condition. Additionally, the independent and combined associations of AF, AIP, and VAI with resting arterial BP remain unexplored in this context. Understanding these relationships is critical for developing strategies to mitigate the rising prevalence of HTN by promoting physical activity, improving fitness, and reducing weight.
Purpose of the study
The purpose of this study was to examine the independent and combined associations of AF, AIP, and VAI with resting arterial BP in Nigerian adolescents. Specifically, the study aimed to: Identify the cardiometabolic disease (CMD) risk factors most strongly associated with HTN risk. Characterize participants’ HTN risk profiles. Determine the independent and combined associations of each independent variable with HTN risk. Determine the predictive capacities of the independent variables for identifying HTN risk among Nigerian adolescents. It was hypothesized that there would be no significant associations between AF, AIP, and VAI levels and the risk of developing HTN.
MATERIALS AND METHODS
Participants
Adolescent participants, both male and female, aged 11 to 19 years, were recruited from secondary schools in Kogi East, North Central Nigeria. This cross-sectional study involved four secondary schools, with a total of 418 adolescents selected using a multistage cluster and random sampling approach. The Slovin formula was applied to determine the sample size, considering a 5% margin of error and a 95% confidence level[27]. Although the minimum required sample size was 399, it was increased to 418 due to enhanced accessibility, to accommodate potential dropouts, and improve representativeness. Participants were selected using a systematic sampling procedure, with every fourth student on the class list included, starting from a predetermined number. The inclusion criteria were as follows: No history of CVD or any reported health issues, no current illness, and no participation in an organized exercise program for at least six months before data collection. A detailed description of the pilot testing procedures have been documented previously[28].
Participants were acquainted with the study purpose and testing protocols after securing approvals from the participating schools. The testing team conducted two visits: The first involved assessing participants' physical attributes and familiarizing them with fitness assessments, while the second included BP and biochemical evaluations alongside fitness testing. To ensure uniformity, all assessments were performed in a standardized sequence by the same evaluators throughout the study.
Study setting
This study was conducted among in-school adolescents in the Kogi East Senatorial District of Kogi State, Nigeria. Kogi State, with its capital in Lokoja, is located in Nigeria’s North-Central geopolitical zone. Secondary schools in Nigeria fall into two main categories: Public and private. Classes typically run from 8:00 am to 2:00 pm. After school hours, children often assist their parents or guardians with various occupations. There is a lack of data on youth fitness and general lifestyle habits in Kogi State, particularly in relation to their health.
Physical characteristics assessment
Height, body weight, and WC were assessed following the methods established by the International Society for the Advancement of Kinanthropometry[29]. These anthropometric parameters were obtained while participants wore minimal clothing and remained barefoot. Body weight and height were determined using a calibrated digital weighing scale (Model Sec-880; Seca Birmingham, United Kingdom) and a wall-mounted stadiometer (Model Sec-206; Seca Birmingham, United Kingdom), with measurements taken to the nearest 0.1 kg and 0.1 cm, respectively. BMI was computed as body weight in kilograms divided by height in meters squared (kg/m2) and was utilized as an indicator of body fat. The percentage of body fat was estimated using triceps and medial calf skinfold thickness, which were assessed with Harpenden skinfold calipers (Creative Health Products, Ann Arbor, MI, United States)[30]. Based on BMI and body fat percentage values, participants were categorized as having a healthy weight or classified as overweight according to the revised Fitness Gram standards[31]. WC, an estimator of abdominal adipose tissue was measured with a Lufkin retractable metal tape (W606PM Rosscraft, Canada) at the level of umbilicus, midway between the lower rib margin and the iliac crest to the nearest 0.1 cm.
AF assessment
AF was evaluated using the 20-meter shuttle run test, a widely recognized multi-stage test for assessing AF in young individuals. Participants ran continuously between two restraining lines set 20 meters apart, adhering to an audio signal. They were encouraged to continue until exhaustion, and those unable to complete two consecutive shuttles were withdrawn from the test. This test is a valid and a reliable measure of AF[32]. The maximum speed attained during the test was used to estimate AF (peak VO2- mL/kg/min) using a prediction equation[31].
Participants were classified into high- and low-fitness groups based on their peak VO2 values, following the revised sex- and age-specific health-related benchmarks of the Fitness Gram[31]. The peak VO2 thresholds were set at 38–43 mL/kg/min for females and 42–52 mL/kg/min for males. Adolescents who met or exceeded these thresholds were categorized as having 'high fitness', while those with values below the cut-off points were classified as having 'low fitness’. Detailed test administration procedures have been outlined previously[31].
BP assessment
Resting SBP and DBP readings were recorded three times at two-minute intervals during morning hours, following a 10-minute seated rest, using an oscillometric device (HEM-705 CP; Omron, Tokyo, Japan). The final BP values were derived from the average of the three readings. BP thresholds for HTN were defined using the 95th percentile for age and sex, based on the criteria established by the National High BP Education Working Group on HTN in Children and Adolescents[12].
Biochemical analysis
Fasting plasma TG and HDL-C levels were determined from capillary blood samples using the Cardio-Check Plus Analyzer (PTS Diagnostics, Indianapolis, IN, United States). The reliability and accuracy of this device have been previously documented[33]. A trained medical team, comprising two nurses and a laboratory technologist, conducted the tests. Participants underwent the biochemical analysis after a 10-minute rest period. Further methodological details have been reported elsewhere[28].
The TG/HDL-C ratio was calculated by dividing TG by HDL-C (mmol/L). To establish a threshold indicative of elevated HTN risk, the sample was categorized into tertiles, with the lowest value of the highest tertile serving as the reference cut-off. In this study, the threshold values were 1.0 for females and 1.1 for males. Given the lack of a universally established TG/HDL-C benchmark for pediatric populations, this method is widely accepted in public health and clinical research[34,35].
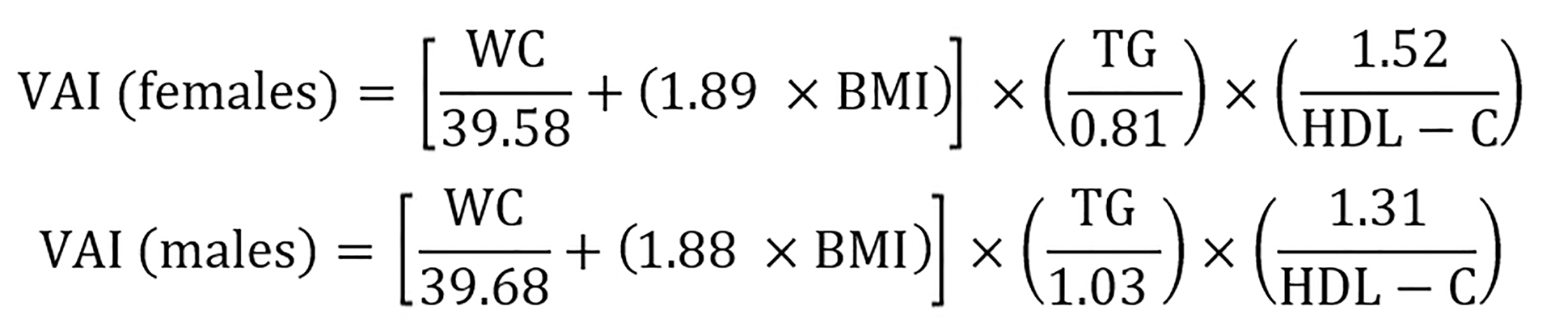
VAI was computed using sex-specific equations formulated by Amato and Giordano[36]:
WC was measured in centimeters, BMI in kg/m2, and lipid values in mmol/L. VAI has been utilized in prior research involving both pediatric[24] and adult populations[19]. Due to the absence of a definitive pediatric VAI threshold for visceral adiposity dysfunction, the highest tertile’s lowest value served as the benchmark[37], which was 1.35 for females and 0.83 for males in this study. This classification approach is widely recognized and employed in epidemiological studies[19,38].
Statistical procedures
Data entry, coding, and statistical evaluations were performed using IBM SPSS Version 20 (IBM Corporation, Armonk, NY, United States). The normality of data distribution was assessed through the Kolmogorov-Smirnov test before conducting further analyses. Descriptive statistics were summarized as means, standard deviations, frequencies, and percentages. Differences based on sex and comparisons between binary groups were analyzed using independent samples t-tests or the Mann-Whitney U test, as appropriate. Pearson’s zero-order correlation was utilized to explore associations between dependent and independent variables. Multivariate regression analyses were employed to investigate relationships between BP and AF, AIP, and VAI. All models were adjusted for chronological age and maturity offset (MO), which was estimated using height and chronological age following the predictive equation by Moore et al[39]. The age at peak height velocity (APHV) was computed by subtracting MO from chronological age. Logistic regression models were applied to assess the independent influence of AF, AIP, and VAI on BP parameters, with separate analyses conducted for male and female participants.
The predictive capacity of the independent variables was further evaluated using receiver operating characteristic (ROC) curve analysis, presenting the area under the curve (AUC) along with a 95%CI. The SBP and DBP thresholds for independent variables were identified as the coordinates with values closest to 1 for the difference between sensitivity (true positive rate) and 1-specificity (false positive rate). AUC values were interpreted according to Hosmer and Lemeshow[40] criteria: AUC = 1 (perfect test), AUC = 0.5 (no discriminative ability), AUC > 0.9 (excellent), 0.8-0.9 (good), 0.7-0.8 (acceptable), and AUC < 0.7 (poor).
Ethics clearance
Ethical approval for the study was granted by the Ethical Review Committee of the College of Health Sciences, Kogi State University, Nigeria (Ref No: COHS/02/25/2020). All participants and their parents/guardians received detailed information about the study objectives and testing procedures. Informed consent was obtained from parents or guardians, and participant assent was secured prior to data collection. The study adhered to the ethical principles outlined in the revised Declaration of Helsinki[41].
RESULTS
Physical and hemodynamic characteristics of participants
The demographic and physiological attributes of participants, categorized by sex, are displayed in Table 1. On average, females exhibited significantly greater body weight (P < 0.001), elevated fat percentage (P < 0.001), MO (P < 0.001), higher BMI (P = 0.021), WC (P < 0.001), VAI (P < 0.001), and elevated SBP (P < 0.001) compared to their male counterparts. Conversely, males demonstrated substantially higher AF (P < 0.001) and advanced APHV (P < 0.001) than females. No significant sex-related differences were observed in chronological age (P = 0.558), AIP (P = 0.091), or DBP (P = 0.143). The overall prevalence of systolic HTN was 5.5%, while diastolic HTN was recorded at 12.7%. Sex-specific prevalence rates are illustrated in Figure 1.
Figure 1 Prevalence of Hypertension risk among participants.
Sys HTN: Systolic hypertension; Dias HTN: Diastolic hypertension.
Table 1 General characteristics of participants stratified by sex (n = 403).
Variable
Total (n = 403)
Girls (n = 201)
Boys (n = 202)
t-value
P value
Age (year)
14.7 ± 2.3
14.8 ± 2.3
14.7 ± 2.2
0.586
0.558
APHV (year)
13.3 ± 1.1
12.5 ± 0.8
14.1 ± 0.8
20.068
< 0.001
MO (year)
1.4 ± 1.3
2.3 ± 1.7
0.6 ± 1.0
10.029
< 0.001
Stature (cm)
160.2 ± 9.8
159.6 ± 7.1
160.9 ± 11.9
0.303
0.193
Weight (kg)
53.1 ± 12.5
55.5 ± 12.1
50.8 ± 12.5
3.784
0.016
BMI (kg/m2)
20.5 ± 3.5
21.7 ± 4.0
19.3 ± 2.6
6.929
< 0.001
WC (cm)
65.8 ± 8.8
67.2 ± 9.4
64.4 ± 8.0
2.273
0.001
20-MST (lap)
32.2 ± 16.8
24.9 ± 13.3
39.5 ± 16.8
9.697
< 0.001
Peak VO2 (mL/kg/min)
40.4 ± 4.4
38.3 ± 4.0
42.5 ± 2.7
10.898
< 0.001
TG (mmol/L)
1.0 ± 0.9
1.1 ± 1.2
0.9 ± 0.4
1.653
0.100
HDL-C (mmol/L)
1.3 ± 0.4
1.3 ± 0.3
1.3 ± 0.4
1.090
0.276
TG/HDL-C
0.9 ± 0.6
1.0 ± 0.6
0.8 ± 0.5
1.697
0.091
VAI
1.2 ± 0.7
1.6 ± 0.8
0.8 ± 0.6
3.912
< 0.001
SBP (mmHg)
105.6 ± 16.7
107.8 ± 16.7
103.5 ± 16.2
2.587
0.010
DBP (mmHg)
69.9 ± 14.5
70.5 ± 15.3
69.5 ± 13.5
0.595
0.552
CVD profile of participants
Table 2 provides a comparative analysis of CVD risk profiles based on systolic HTN classification, dividing participants into "no risk" and "at risk" sub-groups. More females were classified as at risk compared to males. Generally, participants exhibited higher risks of low AF, overweight status, and HTN. For instance, females showed increased risks of overweight status, abdominal obesity, and HTN, while males were more at risk for hypertriglyceridemia. Figure 2 provides additional details on the proportion of adolescents at risk. Evidently, most of the adolescents were at risk of VAT abnormality (56.6%), low fitness (44.4%) and dyslipidemia (33.5%).
Table 3 presents the partial correlation coefficients between the independent variables, SBP, and DBP after controlling for the covariates. Overall, the relationships were weak. For SBP, significant relationships were observed for AF in both sexes and for VAI in females. For DBP, all independent variables were significant (P < 0.05) in males, while only VAI (P < 0.05) was significant in females.
Table 3 Partial correlation coefficients assessing the relationships among aerobic fitness, atherogenic index of the plasma, visceral adiposity index, and blood pressure.
Table 4 outlines the multiple regression models evaluating the predictive capacity of independent variables for SBP, with chronological age and maturity status accounted for. Among females, the covariates in Step 1 did not significantly predict SBP, though they explained 24% of the variance. The inclusion of independent variables in Step 2 increased the total explained variance to 36%, signifying an additional 12% contribution. While all independent variables made unique contributions, VAI (β = 1.439, P < 0.001) had the greatest impact. In the males’ model, age (β = 0.799, P < 0.001) explained 26% of the variance in SBP in step 1. Adding the independent variables in step 2 increased the total explained variance to 36%, with the independent variables contributing an additional 10%. Both AF and AIP made significant contributions, with AF demonstrating greater explanatory power. Table 5 outlines the results of the multiple regression model predicting DBP after controlling for covariates. In females, age (β = 0.620, P = 0.012) explained 25% of the variance in DBP in step 1. The inclusion of independent variables in Step 2 raised the explained variance to 31%, meaning the independent variables contributed an additional 6%. Among these, VAI and AIP made unique contributions, with VAI (β = 1.585, P < 0.001) having the greatest impact. In males, the covariates explained 11% of the variance in DBP, while the independent variables contributed an additional 10%, with VAI being the most significant predictor.
Table 4 Standardized regression coefficients assessing the relationships among Aerobic fitness, Atherogenic index of the plasma, Visceral adiposity index, and Systolic blood pressure.
Sex
Predictor
R2
R2 change
Model 1
Model 2
β
P value
β
P value
Girls
Age
0.356
0.116
0.111
0.650
0.700
0.008
MO
-
-
0.383
0.118
-0.264
0.323
Peak VO2
-
-
-
-
0.328
< 0.001
AIP
-
-
-
-
-0.391
< 0.001
VAI
-
-
-
-
1.439
< 0.001
Boys
Age
0.362
0.096
0.799
< 0.001
2.046
< 0.001
MO
-
-
-0.304
0.142
-0.772
< 0.001
Peak VO2
-
-
-
-
0.548
< 0.001
AIP
-
-
-
-
-0.802
0.029
VAI
-
-
-
-
0.704
0.063
Table 5 Standardized regression coefficients assessing the relationships among Aerobic fitness, Atherogenic index of the plasma, visceral adiposity index, and diastolic blood pressure.
Sex
Predictor
R2
R2 change
Model 1
Model 2
β
P
β
P
Girls
Age
0.306
0.064
0.620
0.012
0.791
0.004
MO
-
-
-0.133
0.585
-0.346
0.212
Peak VO2
-
-
-
-
0.116
0.099
AIP
-
-
-
-
-1.528
< 0.001
VAI
-
-
-
-
1.585
< 0.001
Boys
Age
0.208
0.095
1.129
< 0.001
1.407
< 0.001
MO
-
-
-1.103
< 0.001
-1.524
< 0.001
Peak VO2
-
-
-
-
0.293
0.025
AIP
-
-
-
-
-1.4849
< 0.001
VAI
-
-
-
-
1.984
< 0.001
Results of the binary logistic regression models indicated that AF was the only significant factor in males for both SBP [odds ratio (OR) = 1.1, 95%CI: 1.01–1.15, P = 0.018] and DBP (OR = 1.1, 95%CI: 1.03–1.13, P = 0.001). However, the models for females were not significant for either SBP (P = 0.075) or DBP (P = 0.097).
Predictive values of independent variables for HTN risk
Table 6 presents the results of the ROC analyses of the independent variables for SBP and DBP. For SBP, none of the AUCs were significant in either sex. Conversely, for DBP (Figure 3), the AUCs for AIP and VAI were significant (P < 0.001) in females, while none were significant in males. The thresholds for AIP and VAI were 0.6 and 1.0, respectively.
Figure 3 Sex-specific areas under the curves of fitness, Atherogenic index of the plasma, Visceral adiposity index for Diastolic blood pressure in participants.
AF: Aerobic fitness; AIP: Atherogenic index of the plasma; VAI: Visceral adiposity index
Table 6 Receiver operating characteristics curve analysis for hypertension risk among participants.
Outcome variable
Group
Independent variable
AUC
95%CI
Cut-point
Se
Spe
P value
SBP
Girls
AF
0.616
0.462-0.769
37.1
0.571
0.433
0.149
AIP
0.620
0.436-0.805
0.544
0.571
0.599
0.133
VAI
0.597
0.402-0.793
0.764
0.571
0.701
0.224
Boys
AF
0.597
0.415-0.725
41.169
0.750
0.397
0.130
AIP
0.280
0.143-0.416
0.725
0.250
0.412
0.135
VAI
0.330
0.172-0.488
0.822
0.250
0.340
0.103
DBP
Girls
AF
0.503
0.381-0.625
38.9
0.529
0.313
0.956
AIP
0.696
0.610-0.782
0.556
0.706
0.503
< 0.001
VAI
0.698
0.608-0.787
0.954
0.706
0.413
< 0.001
Boys
AF
0.595
0.448-0.743
41.2
0.529
0.605
0.194
AIP
0.464
0.248-0.649
0.726
0.471
0.400
0.625
VAI
0.507
0.331-0.684
0.823
0.471
0.324
0.919
DISCUSSION
This study examined the cross-sectional association of AF, AIP, and VAI with resting arterial BP among adolescents in North-central Nigeria. The findings indicate a modest prevalence of HTN among participants, with females showing a higher prevalence of both systolic and diastolic HTN compared to males. Overall, a substantial proportion of participants were at risk of low fitness, elevated VAI, and AIP compared to other health indicators, with more females being at higher risk than males. The relationships between the independent variables and SBP were generally weak, with only AF demonstrating a significant relationship with SBP in both sexes and VAI showing a significant association with SBP in females. Conversely, all independent variables were significantly related to DBP in males, while only VAI was significantly related to DBP in females. The independent variables were separately and jointly associated with SBP in both sexes, with VAI having the greatest impact in females, while AF and AIP had stronger impacts in males. For DBP, VAI again made the greatest contribution in both sexes. Females were more at risk of CVD than males, based on stratification by systolic HTN risk. Only VAI and AIP demonstrated diagnostic capacities to identify diastolic HTN in females.
Cardiometabolic characteristics of participants
The prevalence of systolic HTN (5.5%) documented in this study aligns with findings from a previous study on South African adolescents, which reported a prevalence of 4.9%[14]. However, the diastolic HTN prevalence of 12.7% observed in this study is significantly higher than the 6.5% reported for South African adolescents. Similarly, prevalence rates of 3.6% and 19.0% for systolic and diastolic HTN, respectively, reported for Indonesian adolescents[42] differ substantially from the current findings. Notably, the pooled global prevalence of 4% and the African prevalence of 6.94% reported in recent decades[43] are significantly lower than the rates observed in this study, suggesting a rising trend of HTN among adolescents in North-Central Nigeria.
With the exception of HDL-C, all cardiometabolic health indicators were significantly more favorable among adolescents without systolic HTN risk, aligning with previous studies[44,45]. Females were at risk for more adverse health indicators than males, potentially due to earlier average maturation among females, which is associated with higher CVD risks[46]. A substantial proportion of adolescents exhibited increased risk of VAT dysfunction, low fitness, and dyslipidemia, with a larger proportion of females affected. This finding highlights the serious health risks posed by high visceral adiposity, low AF, and blood lipid abnormalities compared to body weight and BP abnormalities in this population (Figure 2).
Associations between health markers and HTN risk
Our findings indicate a weak relationship between AF and SBP in both sexes and between VAI and SBP in females only, consistent with previous research[7]. In this study, more males were at risk of low AF, while more females were at risk of high VAI, explaining sex differences in the impact of these independent variables on BP. This suggests the necessity of a comprehensive assessment of HTN risk factors to identify those most indicative of HTN risk for targeted interventions.
The independent variables were separately and collectively associated with systolic HTN risk, with VAI demonstrating the greatest explanatory power in females, aligning with previous research[24,47]. In males, AF and AIP were uniquely associated with SBP, with AF having the greater impact, corroborating earlier studies in adolescents[13,48,49] and adults[20]. Results for DBP also indicated significant independent and combined associations, with VAI again showing the greatest explanatory capacity in both sexes. These findings underscore the need for multi-factorial interventions to prevent and manage BP risk in adolescents. The joint contribution of AF, AIP, and VAI in predicting BP was modest, explaining 6%-12% of the variance in SBP and DBP. However, the primary predictors of BP were age and sexual maturity, which explained 24%-26% of the variance. These findings have significant public health implications. Previous studies have documented the influence of age and sexual maturation on BP regulation[46,50,51]. It has been observed[46] that adolescents with early maturation have more cardiovascular risk factors, when compared with their peers with late maturation. Furthermore, Cho and colleagues[51] in a study involving 383 adolescents aged 11-16 years, reported that participants advanced in sexual maturity had significantly higher SBP, with DBP predicted by age and BMI in females, and height in males. They concluded that sexual maturity provides important and independent information on BP in adolescents. Recent reviews have also highlighted the positive relationship between sexual maturation and BP, especially SBP, in youth[50,52]. The females’ advanced maturity status in this study may be responsible for their higher vulnerability to HTN risk than males.
The prominence of VAI in predicting BP in both sexes is noteworthy. VAI serves as a proxy for visceral fat accumulation and plays a critical role in the CMD profile, secreting biomarkers that contribute to CMD pathophysiology, including HTN[53]. Excess visceral adiposity may lead to hormonal, inflammatory, and endothelial perturbations, resulting in increased sympathetic activity, renin-angiotensin-aldosterone system (RAAS) activation, endothelial dysfunction, pro-inflammatory cytokines such as C-reactive protein, interleukin-6, tumor necrosis factor-alpha and adipokine such as leptin, all of which contribute to HTN[54]. The unique association of AIP with BP risk is consistent with findings in Italian and Korean adolescents[26,49]. In a study of Korean adolescents, Chu et al[26] identified AIP as an important marker of metabolic syndrome, including BP risk, with high predictive value. These findings highlight the necessity of multi-factorial strategies for HTN prevention and management in adolescents.
The significant association of AF with BP underscores its public health relevance. AF is strongly linked to reduced arterial stiffness, systemic inflammation and oxidative stress as well as improved endothelial function, which regulates vascular tone and health, leading to better BP control[55]. Encouraging regular participation in endurance-type physical activities is consistent with current physical activity guidelines for youth[56] and is essential for reducing HTN risk and promoting cardiometabolic health. Interestingly, other studies have shown that unfavorable levels of AIP and VAI can increase mortality in young adult stroke patients[57]. Moreover, VAI has been identified as a strong correlate and independent predictor of diabetes risk in both adolescent males[47] and females[58], as well as a risk factor for CVD in adolescents[21]. These findings further support the negative health effects of these biomarkers observed in the present study.
Diagnostic utility of AF, AIP, and VAI
In this study, only AIP and VAI demonstrated diagnostic capacities to detect diastolic HTN risk in females, consistent with findings in Iranian and Saudi Arabian youth[24,47]. Although these health indicators show low predictive capacities to detect diastolic HTN, these results suggest that blood lipid abnormalities and high VAT accumulation are significant health concerns in this cohort. Future public health strategies should integrate AIP and VAI assessments into routine health screenings, particularly in school-based settings.
Molecular cytopathological effect of Fitness, lipid ratios and VAI on HTN
HTN is a complex condition influenced by multiple metabolic and physiological factors, including AF, lipid ratios, and the VAI. Each of these factors affects molecular pathways and cellular structures involved in the pathophysiology of HTN[47,48,55]. AF exerts protective molecular effects against HTN by enhancing endothelial function and increasing nitric oxide production, which promotes vasodilation and lowers BP. Additionally, it reduces oxidative stress and inflammation while modulating the RAAS, further contributing to BP reduction. At the cellular level, improved fitness enhances smooth muscle cell relaxation and decreases arterial stiffness, vascular inflammation, and atherosclerotic plaque formation[55].
Conversely, poor lipid ratios and elevated VAI contribute to HTN through endothelial dysfunction, chronic inflammation, plaque development, oxidative stress, increased leptin levels, reduced adiponectin, and overall metabolic dysregulation[23,47,48]. The cytopathological consequences include endothelial damage, arterial stiffening, increased vascular resistance, and heightened inflammatory cell infiltration[54]. These changes accelerate atherosclerosis, impair vasodilation, and promote HTN progression[23]. Therefore, encouraging healthy lifestyle choices such as engaging in regular endurance exercise, eating balanced diet and observing other weight control measures among adolescents are crucial for mitigating HTN risk and improving cardiovascular health.
Public health implications
The modest variance in HTN risk explained by the independent variables still holds significant health implications. The 12% and 10% variance explained for SBP in females and males, respectively, suggests a potential reduction in systolic HTN risk by about one-tenth. Similarly, the 6% and 11% variance explained for DBP in females and males, respectively, highlights the potential for a comparable reduction in diastolic HTN risk, especially in males. These findings emphasize the importance of healthy lifestyles, including balanced diets and regular aerobic physical activity.
The results of this study suggest that higher AF levels and lower AIP and VAI values are associated with better BP regulation. This study also demonstrated that poor fitness has a more pronounced effect on BP in males, while elevated AIP and VAI levels pose greater health risks for females. Given that females are more vulnerable to CVD risk factors as observed in the present study, public health interventions should adopt a sex-specific approach. School- and community-based health initiatives in Nigeria should be tailored to the unique needs of each sex. For females, these programs should emphasize maintaining a healthy lifestyle, including balanced diets and physical activity that specifically reduces visceral fat accumulation. For males, interventions should prioritize AF while promoting healthy dietary habits with less focus on visceral fat reduction. Additionally, public health policies should incorporate routine health screenings to detect CVD risk factors early, focusing on BP levels among adolescents. Such a strategy would enable timely interventions to mitigate HTN and related CVD risks.
Study limitations and strengths
The cross-sectional nature of the study constrains causal interpretations. Moreover, the inclusion of only school-enrolled teenagers restricts the generalisability of the findings to those without formal education, and this may also introduce sampling bias. Furthermore, field-based tests for AF might not be as accurate as laboratory-based techniques like VO2 max measurement. However, the use of AF and BMI health-related thresholds which revealed that meeting health standards correlated with improved BP profiles is a notable strength. Another strength of this study is the direct measurement of study participants which provided more reliable results than self-reported information.
CONCLUSION
This study documents the susceptibility of Nigerian adolescents to the risk of HTN. While low fitness, dyslipidemia, and visceral adiposity dysfunction were independently linked to HTN risk, the association between VAI and HTN risk was particularly high in females. Although the combined influence of independent variables on HTN risk was moderate, age and sexual maturity emerged as primary determinants of BP outcomes. Health promotion initiatives should emphasize balanced nutrition and regular aerobic activity to maintain optimal BP levels, mitigate HTN risk, and enhance long-term cardiovascular health in adolescents, particularly among females. Future longitudinal research is needed to further elucidate the roles of AF, AIP, and VAI in predicting HTN risk in youth.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the cooperation of the school heads, teachers, and students of the participating schools. The authors also gratefully thank the research assistants for facilitating data collection process.
Footnotes
Provenance and peer review: Invited article; Externally peer reviewed.
Peer-review model: Single blind
Specialty type: Pediatrics
Country of origin: Nigeria
Peer-review report’s classification
Scientific Quality: Grade A
Novelty: Grade B
Creativity or Innovation: Grade C
Scientific Significance: Grade B
P-Reviewer: Soltanipur M S-Editor: Liu H L-Editor: A P-Editor: Yu HG
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents.Pediatrics. 2004;114:555-576.
[PubMed] [DOI] [Full Text]
Marfell-Jones M, Stewart AD, de Ridder JH.
International standards for anthropometric assessment. Wellington, New Zealand: International Society for the Advancement of Kinantropometry, 2012.
[PubMed] [DOI]
Cureton KJ, Plowman SA, Mahar MT.
Aerobic capacity assessment. In: Plowman SA, Meredith MD. In FitnessGram?ActivityGram reference Guide. Dallas, United States: The Cooper Institute, 2013: 6-1-6-22.
[PubMed] [DOI]
Gao Y, Zhu CG, Wu NQ, Guo YL, Liu G, Dong Q, Li JJ. [Study on the reliability of CardioChek PA for measuring lipid profile].Beijing Da Xue Xue Bao Yi Xue Ban. 2016;48:523-528.
[PubMed] [DOI]
Al-Daghri NM, Al-Attas OS, Alokail M, Alkharfy K, Wani K, Amer OE, Ul Haq S, Rahman S, Alnaami AM, Livadas S, Kollias A, Charalampidis P, Sabico S. Does visceral adiposity index signify early metabolic risk in children and adolescents?: association with insulin resistance, adipokines, and subclinical inflammation.Pediatr Res. 2014;75:459-463.
[RCA] [PubMed] [DOI] [Full Text][Cited by in Crossref: 35][Cited by in RCA: 44][Article Influence: 4.0][Reference Citation Analysis (0)]
Pireva A, Selimi M, Gontarev S, GEORGI G. Association between aerobic fitness and high blood pressure in adolescents in Macedonia evidence for criterion-referenced cut-points.J Phys Edu Sport. 2018;18:853-861.
[PubMed] [DOI] [Full Text]
Cho SD, Mueller WH, Meininger JC, Liehr P, Chan W. Blood pressure and sexual maturity in adolescents: the Heartfelt Study.Am J Hum Biol. 2001;13:227-234.
[PubMed] [DOI] [Full Text]
Herlina N, Astuti Z, Kustiawan PM. The comparison of visceral adiposity index, fasting triglycerides and glucose index, and triglyceride/ high-density lipoprotein cholesterol ratio as predictors of stroke mortality.Multidiscip Sci J. 2024;7:2025317.
[PubMed] [DOI] [Full Text]